For centuries, the heart was viewed as an autonomous muscular pump remarkably resilient, yet ultimately doomed to age through mechanical […]
Immunology rarely fails loudly, when it misfires, it usually does so subtly and at the margins. mRNA COVID-19 vaccines were designed to exploit the immune system’s most conserved antiviral pathways, activating them briefly and then withdrawing. This design has proven extraordinarily successful, producing strong protection with minimal biological disturbance across billions of recipients.
Within this vast dataset, a narrow signal emerged: transient myocarditis occurring shortly after vaccination, primarily in adolescent and young adult males. The rarity and reversibility of these cases suggested not toxicity, but a regulated immune process temporarily exceeding its intended bounds. The challenge was to identify where regulation loosened.
Stanford Medicine investigators approached this as a problem of immune signal flow. By tracing cytokine activity from innate immune activation through adaptive immune amplification, they identified a specific inflammatory axis involving CXCL10 and interferon-gamma (IFN-γ). In rare individuals, this axis becomes transiently overexpressed, redirecting immune activity toward myocardial tissue and producing short-lived inflammatory injury.
A multidisciplinary research team led by Joseph Wu, MD, PhD, Director of the Stanford Cardiovascular Institute, has now provided important mechanistic insight into this phenomenon. Using advanced immunological profiling, patient-derived data, and experimental models, the investigators mapped the immune signaling pathway that can, under specific conditions, result in heart muscle injury.
Myocarditis is characterized by inflammation of heart muscle tissue and can arise from viral infections, autoimmune conditions, toxins, or immune dysregulation. Clinically, it may present with chest pain, dyspnea, palpitations, fever, or fatigue. Biochemically, myocardial injury is commonly reflected by elevated circulating levels of cardiac troponin, a protein normally confined to cardiomyocytes.
COVID-19 infection itself is a well-recognized cause of myocarditis, with a substantially higher incidence than that observed after vaccination. Nevertheless, the occurrence of myocarditis following vaccination, particularly in the absence of detectable viral infection, raised important questions regarding immune mechanisms specific to mRNA platforms.
The Stanford investigators sought to answer a central question: why do mRNA vaccines, in rare cases, trigger myocarditis in otherwise healthy young individuals?
To address this, the research team analyzed blood samples and clinical data from individuals who had received mRNA COVID-19 vaccines, comparing those who developed myocarditis with those who did not. They employed high-resolution immune profiling techniques, now commonly used in translational immunology, to examine cytokine signaling patterns and immune cell activation states.
This patient-derived data was complemented by experimental modeling to explore causality and downstream tissue effects.
The investigators identified a distinct immunological signature in individuals who developed myocarditis after vaccination. Two cytokines, CXCL10 and interferon-gamma (IFN-γ) were consistently elevated in these individuals.
CXCL10 is a chemokine primarily produced by innate immune cells such as macrophages. It functions as a chemoattractant, guiding immune cells to sites of inflammation. Following mRNA vaccination, macrophages recognize the synthetic mRNA and lipid nanoparticle components as foreign molecular patterns. This recognition is essential for vaccine efficacy, as it initiates immune activation and antigen presentation.
In most individuals, this response remains tightly regulated. However, in susceptible individuals, macrophages produce disproportionately high levels of CXCL10.
CXCL10, in turn, recruits and activates T lymphocytes, particularly cytotoxic and helper T cells. These T cells secrete interferon-gamma, a cytokine that plays a central role in antiviral defense by enhancing antigen presentation, activating macrophages, and inhibiting viral replication.
While IFN-γ is indispensable for effective immunity, excessive or prolonged signaling can be deleterious. The Stanford study demonstrated that elevated IFN-γ levels amplify inflammatory signaling within cardiac tissue, promoting immune cell infiltration and local cytokine release.
The combined activity of CXCL10 and IFN-γ creates a pro-inflammatory microenvironment within the myocardium. Experimental data showed that this environment can directly injure cardiomyocytes by:
This injury is reflected clinically by elevated cardiac troponin levels, confirming cardiomyocyte membrane disruption or cell death.
Notably, the investigators observed that this inflammatory process can propagate further immune activation, creating a feed-forward loop that exacerbates tissue damage, albeit transiently in most cases.
One of the most intriguing aspects of post-vaccination myocarditis is its demographic pattern. The Stanford team explored potential biological explanations for the higher incidence among adolescent and young adult males.
Experimental data suggested that estrogenic signaling may exert a protective, anti-inflammatory effect on cardiac tissue. Compounds such as genistein, a naturally occurring phytoestrogen, were shown in laboratory models to dampen CXCL10 and IFN-γ–mediated inflammation and reduce myocardial injury.
These findings suggest that sex-based hormonal differences may modulate immune responses to mRNA vaccination, though the authors emphasize that this hypothesis requires further clinical validation.
The study also raises the possibility that mRNA-induced cytokine signaling may transiently affect other organs. Prior observations from the Stanford group and others suggest inflammatory changes in tissues such as the lung, liver, and kidney in experimental systems.
While these effects appear subclinical and reversible, they underscore the systemic nature of immune activation triggered by mRNA platforms. Importantly, no evidence suggests long-term organ damage in vaccinated individuals.
The findings from Stanford Medicine carry several important implications:
The absolute risk of vaccine-associated myocarditis remains extremely low, and the risk from COVID-19 infection itself is substantially higher. These findings reinforce not undermine, the favorable risk-benefit profile of mRNA vaccines.
Identifying CXCL10 and IFN-γ as central mediators provides a coherent biological explanation for a previously puzzling adverse event.
The study suggests potential strategies for mitigating myocarditis risk, including modulation of specific cytokine pathways or refinement of vaccine formulations, without compromising immune protection.
Elevated IFN-γ signaling is a fundamental immune response to foreign nucleic acids, implying that similar mechanisms could, in principle, apply to other mRNA-based therapies.
“The mRNA vaccines have done a tremendous job mitigating the COVID pandemic,” said Joseph Wu. “Without these vaccines, more people would have gotten sick, more people would have had severe effects, and more people would have died.”
He emphasizes that immune signaling pathways such as IFN-γ are essential for antiviral defense, but like many powerful biological systems can become harmful when excessively activated.
The Stanford Medicine study represents a major advance in understanding the rare occurrence of myocarditis following mRNA COVID-19 vaccination. By identifying a specific cytokine-driven immune cascade, the research provides mechanistic clarity, reassures vaccine safety, and opens avenues for further optimization of mRNA technologies.
As mRNA platforms continue to expand into vaccines for other infectious diseases and therapeutic applications, such mechanistic insights will be critical for maximizing benefit while minimizing risk. Far from undermining confidence in vaccination, this work exemplifies the self-correcting nature of biomedical science, where rare adverse events are rigorously studied, understood, and addressed to improve outcomes for all.
For centuries, the heart was viewed as an autonomous muscular pump remarkably resilient, yet ultimately doomed to age through mechanical […]

Republic Day is one of the most important milestones in the political and constitutional history of India. Observed annually on […]
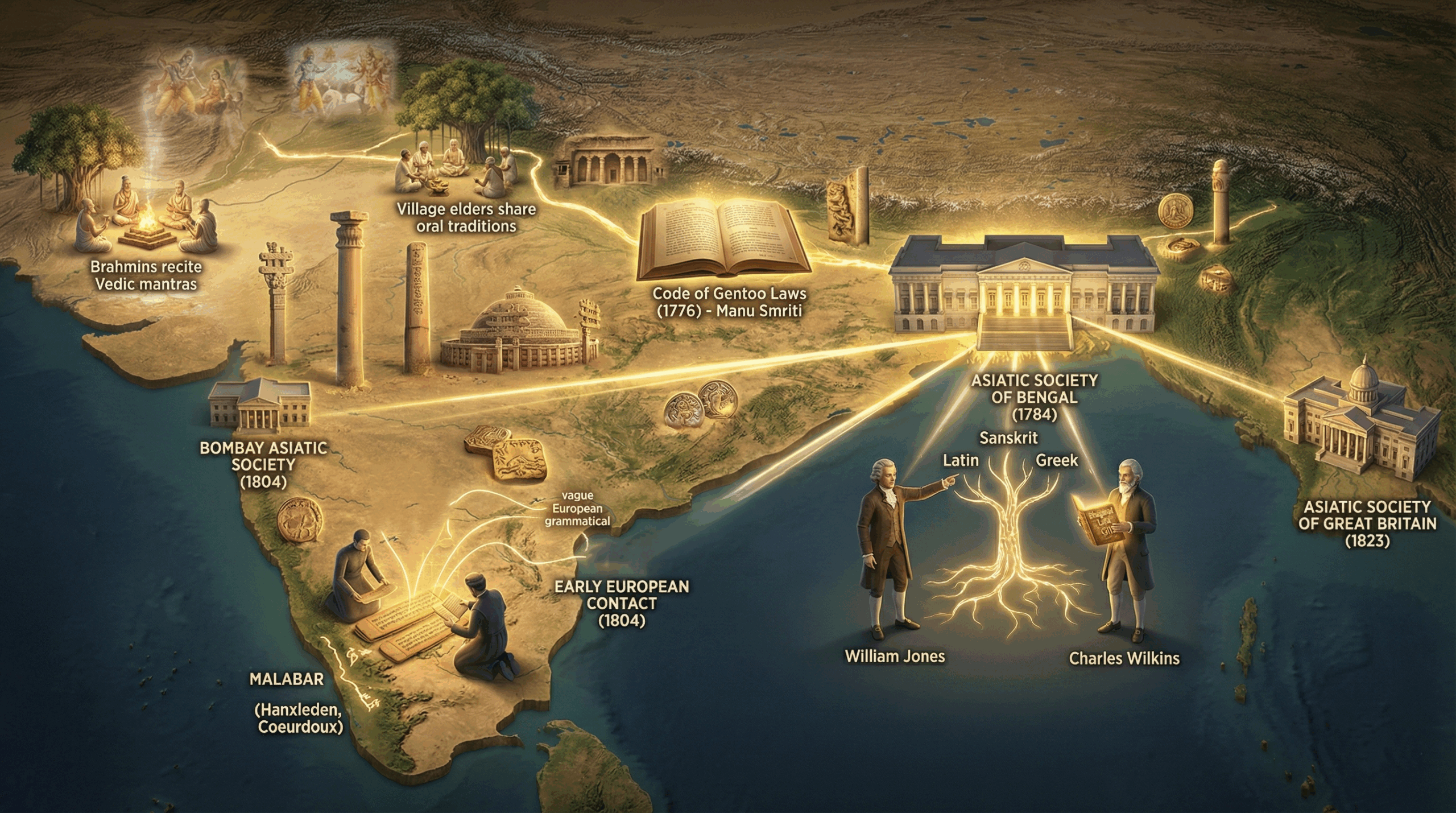
‘How the ancient history of India in modern times came to be noticed’ Introduction Ancient Indian civilization was unlike those […]