
Tobacco smoke has always been treated as something that fades once the air clears. Open a window, turn on a […]
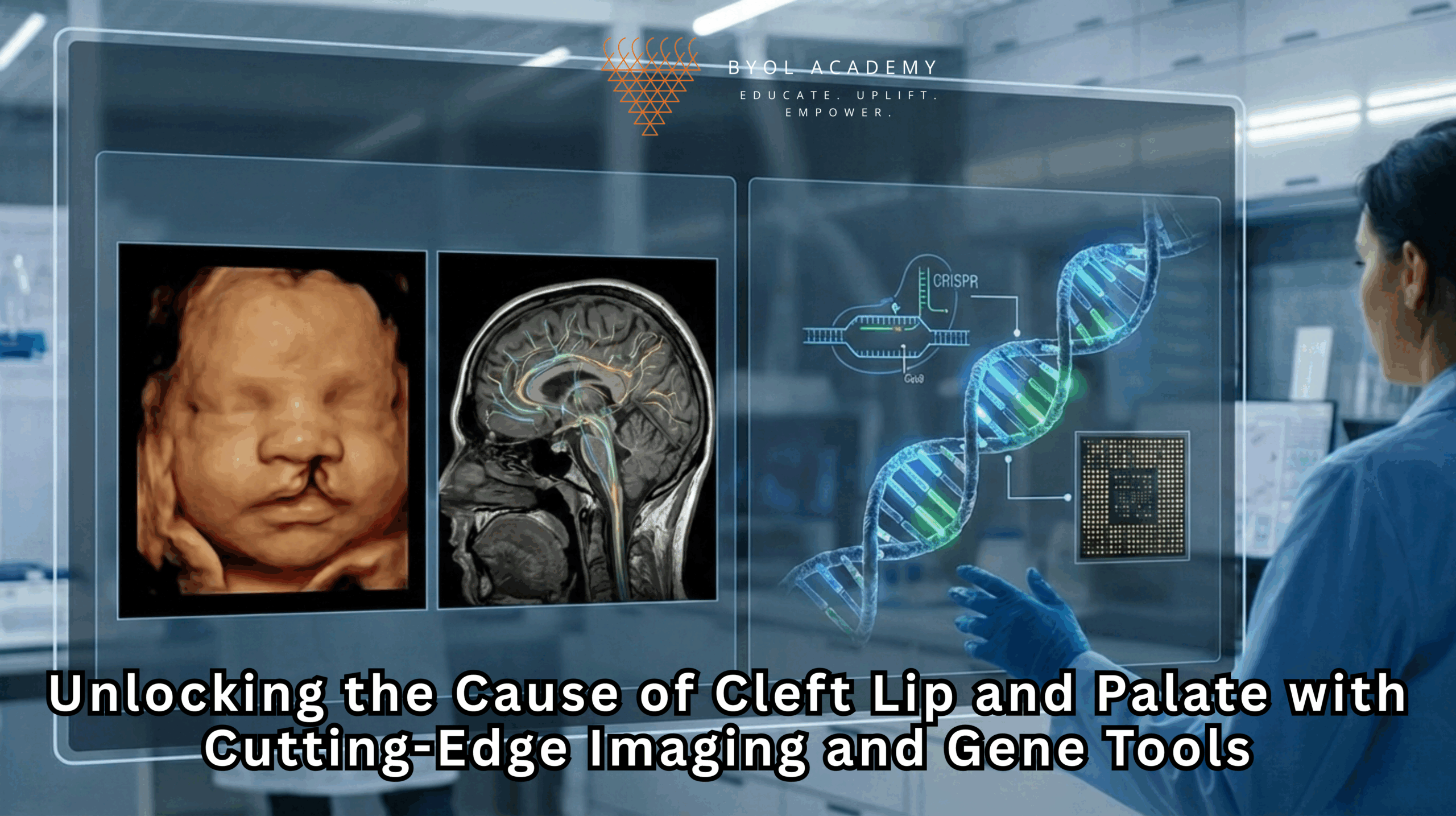
Every face tells its own story. Genetics shapes much of that story, but when key developmental instructions go awry, babies can be born with facial differences such as cleft lip or cleft palate. Without proper treatment, these craniofacial anomalies can interfere with a child’s ability to feed, breathe, see, speak, and maintain ear health, affecting far more than appearance. The scientific challenge has always been to understand why these defects arise in the first place and how we might one day prevent them.
While these anomalies appear as simple gaps or openings, the biology behind them is anything but simple. The story starts in the embryo, long before birth, where tissues must grow, migrate, and fuse with astonishing precision. A single misstep can alter the entire architecture of the face.
At UC San Francisco, Professor Jeffrey Bush, Ph.D., and his research team are piecing together this puzzle by looking directly into the biological events that sculpt the human face during fetal development. Their work traces the earliest steps of facial formation, an intricate process that unfolds in the embryo long before birth.
The Centers for Disease Control and Prevention (CDC) estimates that one in 33 babies is born with a structural birth defect, and cleft lip and cleft palate occur in roughly one in 700 births. This makes them the fourth most common congenital anomaly in the United States.
A cleft lip forms when the two halves of the upper lip fail to fuse during early pregnancy. A cleft palate occurs when the tissues that form the roof of the mouth do not properly join, leaving an opening that may extend from the front teeth to the throat.
Surgery can correct the physical defect, but it does not solve the underlying biological cause. Nor does it prevent the need for multiple operations as the child grows. This gap between treatment and prevention is precisely where Bush’s research begins.
The human face does not form as a fixed structure. Instead, it emerges through a carefully timed choreography of growth, movement, and fusion of distinct embryonic regions called facial prominences. These include:
Between weeks 4 and 10 of human gestation, these structures expand, curve, and migrate. Eventually, they meet at precise angles and fuse, sealing the upper lip and palate.
If the timing or movement of even one cell population is off by hours, fusion can fail.
Historically, this process was nearly impossible to study directly because it occurs deep within the embryo, involves microscopic tissues, and happens rapidly. Developmental biologists relied on fixed tissue slices, essentially snapshots that freeze time. These images showed the beginning and the end of fusion but not the dynamic activity in between.
Live imaging has changed everything.
Using advanced microscopy platforms, Bush’s team can now record time-lapse videos of facial fusion in mouse embryos, capturing images every 15–20 minutes over many hours.
This technique provides an unprecedented view of facial development:
Fusion events can be monitored frame-by-frame.
These recordings reveal that lip and palate formation follow a zipper-like model of fusion. Two tissues advance toward each other, align with extreme precision, and then merge through a coordinated series of cell movements.
Failures in this zipper mechanism account for many clefting events.
Bush’s group identified several crucial biological processes involved in bringing the two sides of the lip together:
1. Cell Adhesion and Molecular Anchoring
Cells rely on adhesion proteins to attach to one another. Without this anchoring, tissue surfaces cannot grip and fuse.
One key player is CDH3, a cadherin molecule that ensures cells bind with adequate strength. Mutations or disruptions in CDH3 weaken adhesion and make fusion mechanically unstable.
2. Actomyosin Contractility
Cells generate pulling forces using actomyosin fibers, protein filaments that act like microscopic springs. These forces:
Bush’s live imaging revealed a “force threshold” that must be met for successful fusion.
3. Directed Cell Migration
Cells do not drift randomly. They follow molecular cues that guide them across the fusion zone. Interrupting these signals can halt migration, leaving a gap.
4. Epithelial Seam Breakdown
After the two sides meet, a temporary seam of cells must disassemble. Failure to dissolve this seam prevents complete closure.
Together, these processes form a multi-layered system. Cleft lip or palate emerges when any part of this system falters.
Live imaging shows how fusion occurs. Gene editing helps answer why it sometimes fails.
Bush’s team uses CRISPR-Cas9 to introduce specific gene mutations, mirroring those found in human infants, into mouse embryos. They then use live imaging to observe the exact cellular consequences.
This approach bridges three levels of biology:
Genetic: which DNA changes increase risk
Cellular: how cells behave differently
Tissue-level: how fusion fails in real time
CDH3 mutations were among the most revealing. Mice with altered CDH3 showed malformed adhesion structures and incomplete lip fusion, mimicking the cleft phenotype.
These experiments create a direct link between clinical genetics and embryonic development, a powerful tool for diagnosing and understanding clefting risks.
The Bush lab’s most influential study, published in the Journal of Cell Biology, demonstrated:
Postdoctoral researcher Camilla Teng produced the breakthrough time-lapse films. Her work documented every stage of fusion with unprecedented clarity and revealed that even slight perturbations in molecular signals can derail the entire process.
This research does more than explain cleft formation, it provides a framework for studying all developmental fusion events, including those involved in cardiac formation, neural tube closure, and organ structure.
The genes involved in craniofacial development do not retire after birth. They continue to function in:
tissue repair
cancer progression
cell migration
wound healing
organ regeneration
Understanding how these genes behave during development helps scientists understand how they may malfunction later in life.
For example:
This makes craniofacial biology a powerful model for broader medical research.
The long-term goal is to move beyond surgery and develop early interventions that support proper development before birth. The path forward includes:
While prenatal treatments are not yet available, Bush’s work is building the scientific foundation needed to make them possible.
From static snapshots to dynamic, real-time visualization, the study of craniofacial development has undergone a revolution. Live imaging and gene editing have turned once-invisible embryonic events into observable processes. The work of Jeffrey Bush and his team is revealing the intricate mechanics of lip and palate fusion at a level of detail never before achieved.
By clarifying how genes shape cellular behavior and how cellular behavior builds the face, this research is leading the field toward a future where cleft conditions may be prevented rather than repaired.
As the science deepens, the possibility of developing precise, targeted, early-life therapies becomes increasingly realistic. What was once hidden at the microscopic heart of development is now coming into view, offering new hope for infants born with craniofacial differences and new insights for medicine as a whole.
Tobacco smoke has always been treated as something that fades once the air clears. Open a window, turn on a […]
Recent developments in regulatory science have marked a pivotal moment for hepatology and clinical research. The U.S. Food and Drug […]

Triple-negative breast cancer (TNBC) remains one of the most clinically challenging forms of breast cancer, defined by the absence of […]