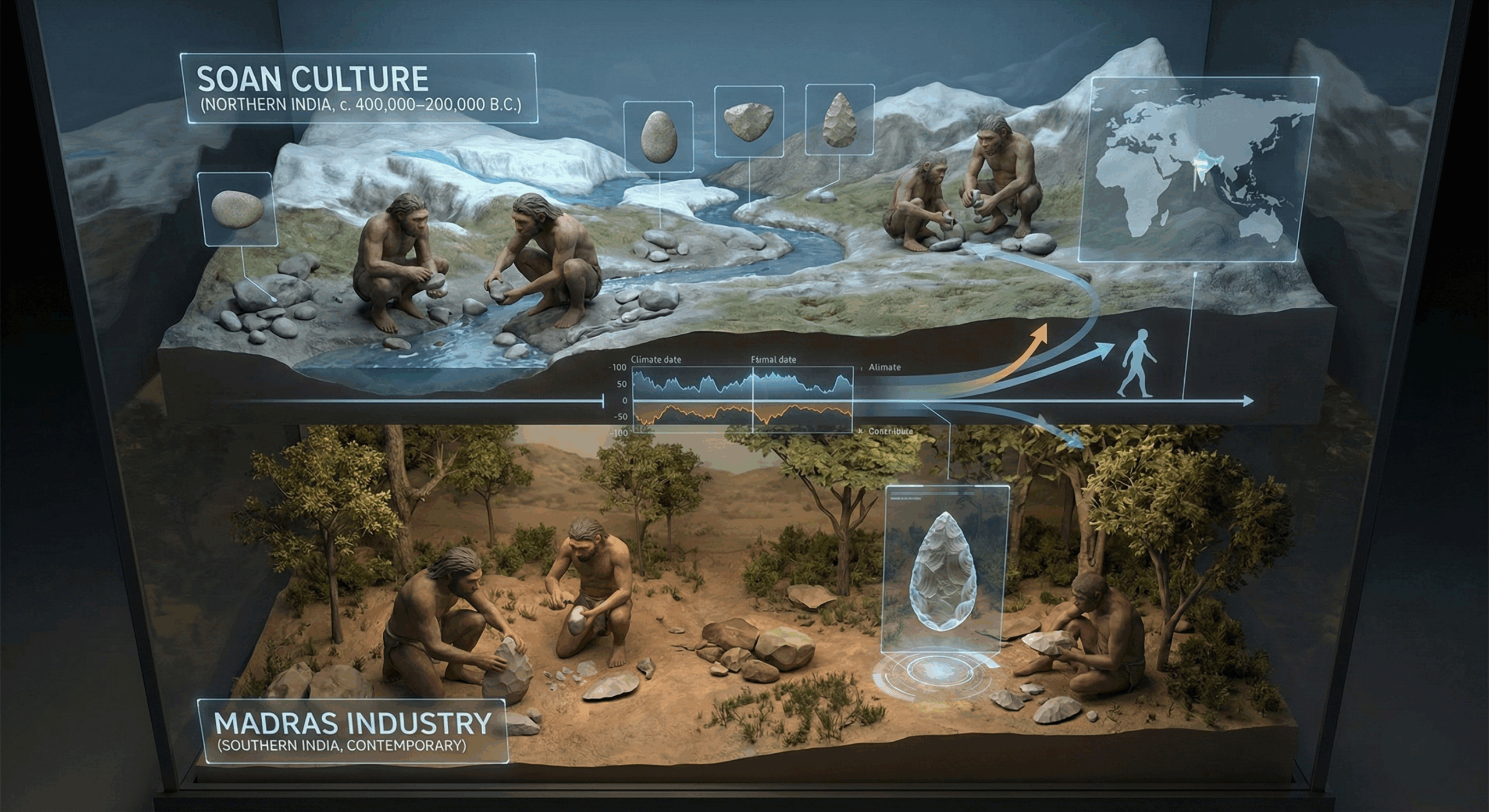
The Soan and Madras industry related to stone age times in Indian sub-continent.

The Rh-null or “golden blood” phenotype is an extraordinary immunohematological condition characterized by the complete absence of all Rh system antigens from erythrocyte membranes. With fewer than 50 known individuals worldwide, Rh-null remains the rarest and most valuable blood type known to medicine. Its immunological universality within the Rh system makes it a potential lifesaver for patients with complex Rh antigen profiles, while its scarcity presents significant transfusion challenges. This review discusses the genetic etiology, biochemical features, clinical manifestations, and global transfusion implications of the Rh-null phenotype, emphasizing its scientific and humanitarian significance.
Blood group systems form the foundation of transfusion medicine, with the ABO and Rh systems being the most clinically significant. The Rh system, comprising over 60 antigens, plays a crucial role in hemolytic disease, transfusion compatibility, and erythrocyte membrane integrity.
Among these, the Rh-null phenotype represents the complete deletion of all Rh antigens — including D, C, c, E, e, and others — on the red blood cell surface. First described in 1961 in an Aboriginal Australian woman, this discovery transformed understanding of Rh antigen biology and membrane physiology. Due to its extreme rarity and scientific value, Rh-null has been termed “golden blood.”
Rh-null blood is estimated to occur in approximately 1 per 6 million individuals. To date, fewer than 50 confirmed cases exist globally.
These individuals belong to various ethnic backgrounds, confirming that the phenotype is not ethnicity-restricted. The International Rare Donor Panel (IRDP) maintains registry coordination to facilitate Rh-null transfusion requests worldwide, emphasizing the need for global donor surveillance and cryogenic storage.
The Rh-null phenotype arises through two principal genetic mechanisms:
Loss of RHAG function disrupts erythrocyte membrane stability, altering cation transport and increasing osmotic fragility. This defect also provides key insights into the functional role of Rh proteins in gas transport and cellular homeostasis.
While some Rh-null individuals remain asymptomatic, others exhibit hematological and morphological abnormalities due to altered membrane architecture:
During systemic infections, hemolytic crises can occur, occasionally progressing to acute kidney injury due to free hemoglobin deposition.
Rh-null blood is considered the universal donor for patients with rare Rh variants because of its complete antigenic neutrality. However, the recipients with Rh-null blood face life-threatening challenges — they can only receive Rh-null blood.
This duality makes Rh-null both medically priceless and clinically precarious.
Blood Phenotype Approximate Frequency Key Features / Clinical Note
Compared to other rare phenotypes, Rh-null remains unparalleled in its antigenic absence and resultant challenges.
Advances, Research & Future Directions
Rh-null blood has become a cornerstone for molecular hematology and membrane biology research. Studies using Rh-null erythrocytes have provided insights into:
Thus, Rh-null blood is not merely a medical rarity but a biological model system for studying red cell physiology and antigen expression.
The Rh-null (“golden blood”) phenotype epitomizes the intersection of rarity, scientific intrigue, and humanitarian importance in modern transfusion medicine. While its universal compatibility within the Rh system offers unparalleled therapeutic potential, its scarcity imposes immense logistical and ethical challenges.
Ongoing genetic research, enhanced rare donor registries, and advanced preservation technologies are imperative to ensure that this “golden” gift of nature continues to illuminate the frontiers of hematology.
The Soan and Madras industry related to stone age times in Indian sub-continent.
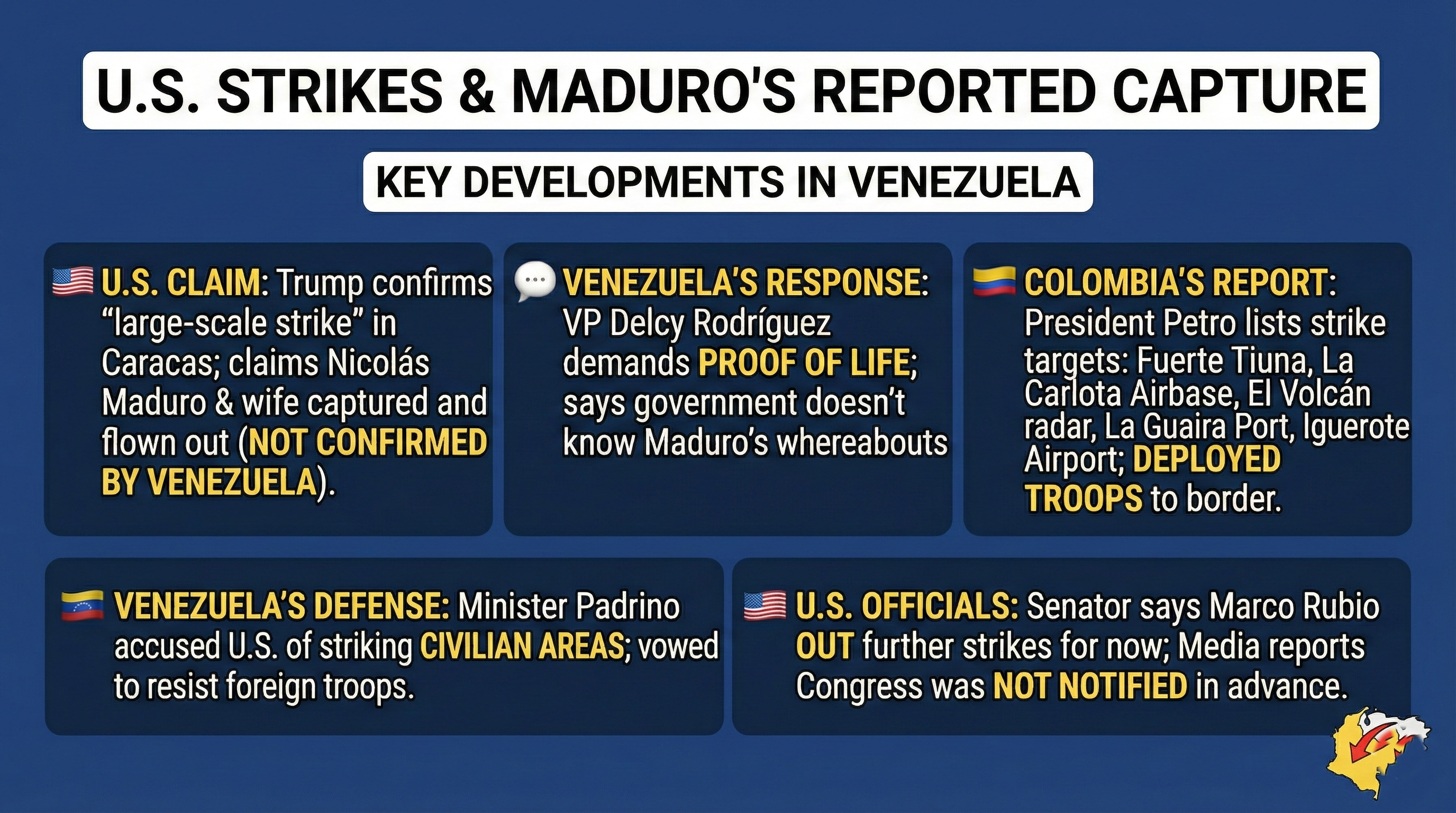
A time bound account of sanctions disputed elections counter narcotics justification. And the January 2026 US air strikes on Caracas. […]
Aging is accompanied by a progressive decline in immune function, a phenomenon that significantly increases susceptibility to infections, diminishes vaccine […]